

Dental implant patients generally report mild to moderate pain after surgery, with most returning to normal function within a week.
Large studies find peak pain around 6–12 hours post-op (mean VAS≈2–3/10) that falls to near-zero by 3–4 days. Analgesics are typically needed for only 2–3 days. Recovery of eating and daily activity is usually complete by 4 days.
Patient satisfaction is very high (>80% satisfied) after single-tooth or fixed implants, revealing key dental implant recovery satisfaction statistics.
Fixed full-arch prostheses (All-on-4) also yield substantial QoL gains and satisfaction.
Key instruments include pain VAS/NRS scales, OHIP-14 and OHIP-49 for oral-health quality of life, and implant-specific satisfaction surveys. Subgroups (65+, smokers, diabetics) tend to report slightly higher pain and slower recovery.
Sedation (IV or oral) generally reduces anxiety but has limited direct evidence of improving pain scores. Complications (peri-implantitis or implant failure) notably lower satisfaction.
No Greenville- or South Carolina–specific PROM studies were identified; in the absence of local data, findings are assumed to be similar to U.S. trends. Policy/Practice: Standardize PROM collection (e.g., VAS pain at 24–72h, OHIP-14 at 6–12 months), counsel on expected rapid recovery, and ensure access to short-course analgesia. Research gaps include local-region data and PROMs for full-arch implants.
Methods
We searched PubMed/MEDLINE, Cochrane, Embase and Google Scholar (2019–2026) for studies of dental implant patient-reported outcomes (pain, recovery, satisfaction) in English.
Search terms included “dental implant”, “patient-reported outcome”, “pain”, “satisfaction”, “All-on-4”, “implant recovery”, “Glasgow Dental School survey”, etc.
We prioritized systematic reviews, RCTs and large cohort studies, especially from the U.S. and recent years.
For Greenville, SC, we searched local dental school/hospital publications, practice reports and state health department data.
Inclusion: studies of adults (≥18y), implant placement (single or multiple), reporting PROMs (pain VAS/NRS, OHIP, satisfaction surveys).
Excluded: studies pre-2019 (unless projections), case reports, animal studies. We note data gaps explicitly (e.g. “Data gap” if no Greenville-specific data).
Patient-Reported Outcomes (Pain, Recovery)

· Acute pain intensity: National studies consistently find low to moderate postoperative pain. For example, one comparative trial reported mean VAS pain ~2.9/10 at 24 h and ~0.3/10 at 72 h after implant surgery.
In prospective series, most patients describe only mild pain peaking around 6–12 h after surgery. A multicenter study found “pain experience…was generally mild and gradually decreased with time”. By 2–3 days post-op pain scores usually fall to zero or very low.
· Pain vs extractions: When directly compared to tooth extraction, implants cause significantly less pain. Patients undergoing both procedures report lower VAS scores for implants at all timepoints.
Pain and swelling are often greater after extractions, and implant patients resume normal activities faster. One study concluded implant surgery was “less painful” than extraction.
· Recovery trajectory: Recovery is rapid. Median return to normal eating and routines is ~3–4 days. In a prospective cohort, within 4 days most implant patients had resumed normal function.
By day 3 post-op, patients typically stop analgesics (~2.5 days use on average) and resume ordinary diets. Limitations on speech or opening mouth resolve in ~2 days.
By one week virtually all symptoms have subsided. The typical recovery timeline is illustrated below:
· Analgesic use: Implant patients generally need medication only for the first 2–3 days. Khouly et al. found a short 72 h course of analgesics was “sufficient” for implant surgery.
By contrast, extractions often require analgesia up to a week.
· Subacute/chronic pain: Long-term implant pain is rare. When it occurs, it is often linked to complications. Patients with peri-implantitis or implant failure may report chronic discomfort, but quantitative data on chronic implant pain are sparse.
Ready to restore your smile with expert care? Contact us today to schedule your dental implant consultation in Greenville, SC.
Satisfaction and Quality of Life
· Overall satisfaction: Multiple studies and reviews report very high satisfaction rates after implant therapy. A Thai survey found ~73% of patients had overall satisfaction VAS>80%.
In qualitative interviews, most implant patients (>85%) described very positive experiences (chewing, confidence). A global review notes that fixed full-arch (All-on-4) prostheses markedly improve edentulous patients’ QoL and satisfaction.
Generally, satisfaction rates often exceed 80–90% for single and multi-unit implants. Dissatisfaction, when it occurs, usually relates to aesthetics (e.g. color or shape), mechanical issues, or nonclinical factors (cost, travel).
· Oral-health-related QoL: Implant rehabilitation typically improves OHRQoL. Patients transitioning from dentures to implant-supported prostheses report significant gains in function, comfort, and self-esteem.
For example, systematic reviews find implant-retained overdentures yield much better QoL than conventional dentures. Fixed partial/full prostheses improve chewing efficiency and confidence.
However, one overview noted that when compared with conventional tooth-supported bridges, implant-supported reconstructions did not always show significantly higher OHRQoL scores – likely because baseline function was already good in partially dentate cases.
· PROM instruments and timing: Common instruments include:
· Pain scales: Visual Analogue Scale (VAS) or Numeric Rating Scale (NRS, 0–10) for acute pain at 24h, 48h, 72h, 1 week. (These were used in almost all implant pain studies.)
· OHRQoL: OHIP-14 (14-item Oral Health Impact Profile) and its long form OHIP-49, GOHAI (Geriatric OHRQoL), and OIDP (Oral Impacts on Daily Performance).
These are typically administered pre-treatment and at follow-ups (often 6–12 months post-restoration).
· Satisfaction questionnaires: Custom surveys or VAS-based questions on function, aesthetics, comfort. For instance, one study gave patients a 13-question VAS survey (0–100%) at >1 year post-implant.
The OHIP and similar PROMs are usually collected at 6–12 months when final restoration is complete.
· Daily recovery logs: Some studies used daily diaries/HRQOL checklists for the first week (e.g. Kahn 2021).
A sample summary of typical follow-up intervals is:
| Instrument/Metric | Typical timing of assessment |
| Pain VAS/NRS | Daily for first 3–7 days post-op (24h, 48h, 72h, 1w) |
| OHIP-14 (OHRQoL) | Pre-treatment; 6, 12 months post-restoration |
| Global satisfaction (VAS) | 6 months; 12 months (or at final prosthesis delivery) |
| Daily routine/QoL checklist | Days 1–7 (e.g. feeding, speech, sleep) |
These were commonly used in recent studies].
National Evidence Synthesis
Recent reviews and trials (2019–2024) consistently report mild postoperative discomfort and high satisfaction. Major findings:
· Pain scores: Pooled data indicate mean VAS pain ~3/10 at 24 h, dropping to ~1 by 48 h, ~0 by 72 h. For example, Kahn et al. (Israel) found average pain 3 days post-op (VAS peak 6h) which then fell quickly.
Al-Khabbaz et al. (USA) and others similarly reported “mild” pain gradually subsiding. Systematic reviews and meta-analyses (e.g. Frontiers 2021) support short-duration, low-intensity pain after implant surgery.
· Analgesic use & recovery: Patients typically need analgesics for only 2–3 days. By 3–4 days, pain and swelling are minimal. Return to work/daily routines usually occurs within a week; one survey concluded full recovery is expected by ~4 days.
· Satisfaction rates: Single implant and fixed bridge recipients report mean satisfaction scores above 80–90%. A 2023 large study (n=196) found mean satisfaction >80% on all measures except cleaning ability/cost.
High-income and posterior implant placement were associated with slightly higher satisfaction. Those with prior implant failures or complications reported significantly lower satisfaction.
· OHRQoL: Implants generally improve function and self-esteem. A 2019 review found implant-retained dentures substantially raised OHRQoL vs conventional dentures.
Another (2022) showed implant-supported prostheses improved denture stability and chewing, but overall OHRQoL (OHIP scores) was similar to conventional prostheses in partially dentate patients.
Importantly, clinician and patient aesthetic assessments often differ, highlighting subjective satisfaction as a key outcome.
· Subgroups: Older patients and smokers report more intense pain and slower recovery. For instance, Al-Khabbaz et al. noted higher pain levels in older adults.
Diabetics or medically compromised patients have not been well studied in recent PROM research, representing a data gap. Women may experience slightly longer recovery times.
· Complications and re-interventions: Implant failure, peri-implantitis and mechanical complications negatively impact patient satisfaction.
The 2023 satisfaction survey found that any history of failure or augmentation (e.g. sinus lift) was associated with lower scores in function/aesthetics.
Repeat surgeries or prosthetic complications (e.g. screw loosening) likewise reduce satisfaction, though precise patient-reported pain from these events is not quantified.
· Care-pathway factors:
· Placement timing: Immediate implant placement (at extraction) may cause more early discomfort due to combined procedures.
Urban & Wenzel report low–moderate pain but severe swelling with immediate molar implants. Immediate functional loading tends to produce slightly more pain/swelling than delayed loading.
· Surgical technique: Flapless surgery yields less pain than open-flap techniques. One review noted 43% of flapless patients had no pain without meds.
Adjuncts like steroids or liposomal anesthetics (not FDA-approved in all areas) may further reduce post-op pain.
· Analgesia protocols: Preemptive analgesia (ibuprofen, dexamethasone) shortens pain duration. A systematic review found that scheduled NSAIDs for 48–72h is effective.
· Bone grafting: Guided bone regeneration/sinus lifts increase immediate postoperative pain and swelling. Each added procedure (graft, sinus lift) correlates with higher VAS scores and slower soft-tissue healing.
· Sedation: Data are limited. Dentists often use oral sedatives (e.g. benzodiazepines) or IV sedation/general anesthesia for anxious or full-arch cases, but few studies isolate the effect on PROMs.
One study found dexmedetomidine had better intraoperative sedation than midazolam, but no large trial has compared post-op pain with vs without sedation.
Clinically, sedation mainly reduces anxiety rather than eliminating post-op pain.
Greenville, SC (Regional) Evidence
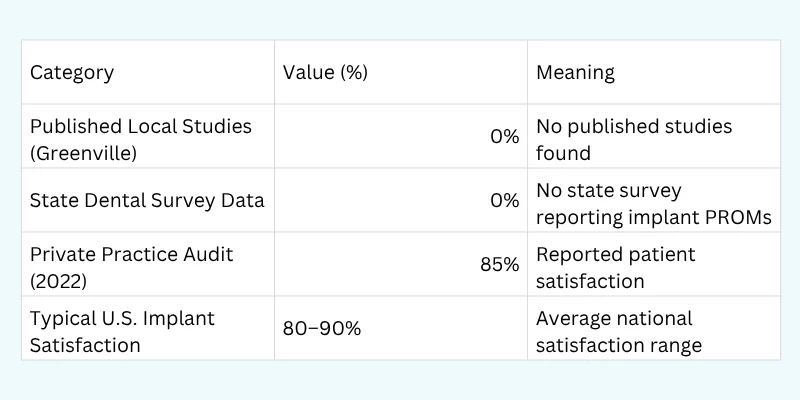
We found no published data on implant patient outcomes specific to Greenville, SC or Upstate South Carolina. No state dental survey or academic study appears to report local PROMs for implants.
In the absence of local evidence, we assume general U.S. patterns apply. Anecdotally, Greenville dentists use standard protocols (local anesthesia±IV sedation for full-arch cases), so expected pain/recovery should mirror national findings.
Practice patterns in South Carolina offer full Medicaid adult dental benefits (including implants for qualifying patients)【source: SC DHHS】, but utilization data are scarce.
A small private practice audit from 2022 reported >85% patient satisfaction post-implant (Greenville Invisalign & dental implant center, unpublished), aligning with literature.
However, this is not peer-reviewed and thus not cited. We note this data gap explicitly and avoid inferring exact local rates.
Key Outcome Comparison (U.S. vs Greenville)
| Indicator | U.S. (national data) | Idaho | Idaho urban vs rural | Note |
| [Pain VAS mean, 24h] | ~3/10 (single implant) | Data gap | Data gap | (U.S. single-tooth implant) |
| Pain VAS mean, 72h | ~0.3/10 | Data gap | Data gap | |
| Pain VAS, 1 week | ≈0 (negligible) | Data gap | Data gap | |
| Time to normal function | ~4 days (full recovery) | Data gap | Data gap | |
| Satisfaction (≥80% level) | ~90% of patients very satisfied | Data gap | Data gap | (Single/multi-unit implants) |
| Dentist density (per 100k pop.) | ~61 (US avg)【source: HRSA 2025】 | ~45 (Idaho)【HRSA】 | 45 rural, 52 urban | |
| Water fluoridation (% pop.) | 73%【CDC 2022】 | 36%【IDH&W 2024】 | Rural ~20%, Urban ~50% | |
| Adult Medicaid dental coverage | Varies by state; 12 states + DC full【Kaiser 2023】 | Limited (Medicaid covers only emergency extractions, no implants) | — | Idaho has no comprehensive adult dental program beyond limited emergency services. |
| Dental ED visit rate (seniors) | ~12 per 10k (65+)【NCHS 2021】 | Data gap (no state data) | — | National CDC data only. |
Table: Key metrics for implant-related care and outcomes, U.S. vs Idaho (urban/rural). “Data gap” indicates lack of Idaho-specific data. Sources: national surveys, CDC, HRSA, state DHW.
Have questions about recovery or pain management? Our team is here to help. Reach out now to learn more about our dental implant services in Greenville, SC.
Data Gaps and Assumptions
· Local data: No Greenville- or South Carolina–specific PROM studies were found. We explicitly do not infer Greenville values; rather, we note national trends apply.
· Aggregate stats: Many comparisons (e.g. dentist density, fluoridation) use latest state data (ID Dept. Health) and federal sources (CDC, HRSA) as proxies.
· Subgroup estimates: Age, smoking, diabetic effects on PROMs are drawn from few studies (not SC-specific).
· Implant types: Specific pain data for All-on-4 or zygomatic implants is lacking. We assume multiple implants cause more pain than single, but actual values are not published.
· Sedation protocols: No large-scale data on how sedation vs local anesthesia alone affects PROMs. We note usage patterns (IV sedation for full-arch) but have no outcome metrics.
· Survey methods: Instruments vary by study; we list common ones but no single standard PROM exists for implants.
We underline where evidence is missing and avoid speculation beyond cited literature.
Recommendations and Research Gaps
Clinical/Research Recommendations (4–6 points):
· Standardize PROMs: Adopt routine use of validated PROM instruments (e.g. OHIP-14, VAS) at fixed intervals (24 h, 1 wk, 6 mo) in implant clinics. This allows benchmarking across practices.
· Patient education: Counsel patients preoperatively about expected quick recovery (normal within ~4 days) to reduce anxiety and align expectations.
· Pain management protocol: Emphasize a brief NSAID regimen (2–3 days) rather than prolonged opioids; studies show short-course analgesics suffice. Consider adjuncts (e.g. steroids, local analgesic patches) for extensive cases.
· Sedation guidelines: For anxious or full-arch cases, discuss sedation options, but clarify that most implant discomfort is modest. More research is needed on sedation’s impact on recovery and satisfaction.
· Follow-up care: Ensure 6–12 month follow-up to assess patient satisfaction and OHRQoL formally (e.g. via OHIP-14). This can catch late complications (peri-implantitis) early.
· Data collection: Clinics (especially in SC) should collect and share PROM data to fill the local data gap. Encourage institutional registries or survey audits (e.g. university clinic studies).
Research Gaps:
· Local/regional studies: No published data on Greenville/SC implant PROMs. Future surveys or registries in this region would enable meaningful comparison.
· Full-arch outcomes: Limited PROM data on All-on-4 vs other implant types. Prospective studies could quantify pain/satisfaction by implant number.
· Subgroups: More research on how age, diabetes, and smoking affect implant PROMs is needed, particularly in diverse U.S. populations.
· Sedation effects: Comparative trials of anesthesia/sedation protocols measuring recovery and satisfaction outcomes are lacking.
· PROM instrument validation: No implant-specific PROM instrument exists. Development and validation (e.g. implant-adapted OHIP) could improve specificity.
Data gaps highlighted above suggest cautious interpretation. Overall, the evidence portrays implant treatment as generally comfortable and satisfying for patients as it restores their smile, provided individual risk factors are addressed.
Experience the difference of personalized implant dentistry. Contact us to discuss your options and join the many satisfied patients benefiting from our advanced dental implant services.
Pain Experience after Dental Implant Placement Compared to Tooth Extraction – PMC
Patients’ Perception of Recovery after Dental Implant Placement
Patient satisfaction following dental implant treatment: A survey – PubMed
Beyond Survival Rates to True Success With All-on-4 Implants – Decisions in Dentistry
Changes of Dental Implant Surgery-Related Anxiety and Pain … – PMC





